The Health and Safety Executive (HSE) is getting ever closer to the release of its new analysts’ guide – intended to help analysts and their clients comply with the Control of Asbestos Regulations 2012 and its Approved Code of Practice (ACoP). I’m reliably informed it will be coming in the next month or two. I know we have all heard this before, but it really does seem to be imminent now.
UPDATE – May 2021: The guide is now published. Click here to download the Analysts’ Guide from the HSE website.
As I highlighted in my review of last November’s FAAM conference, there are some important changes to the guide’s personal monitoring section. These add to an impression that the HSE is taking personal monitoring increasingly seriously, and trying to get to the bottom of why it is generally done so poorly.
If you are struggling to wrap your head around personal monitoring, be reassured that it is a complex subject that often feels academic, with no practical benefit. And if it makes you feel any better, be aware that not everyone at the HSE understands it fully either.
Be careful what you ask for
In regard to personal monitoring, the HSE seems to be asking ‘why do we never get what we ask for?’. In my view, the reason is that the whole subject has never really been communicated with people on the ground (the actual doers) in mind. Here’s an extract from the draft new analysts’ guide:
| Test | Sample Rate (l/min) | Minimum Volume | Minimum Graticules | Resulting LoQ |
| 4-hour Control Limit | 1-2 | 240 | 100 | 0.04 f/ml |
| 10-minute short term exposure limit | 4 | 40 | 100 | 0.24 f/ml |
| Specific short duration activity | 4 | 120 | 100 | 0.08 f/ml |
| Assessment of suitability of RPE | >0.2-4 | 40 | 100 | 0.24 f/ml |
First, a quick explanation for those of you not familiar with the terminology:
Graticules – if you have ever looked down an analyst’s microscope, a graticule is the little target. Stating how many graticules is effectively a statement as to how long / hard an analyst should read the slide. The longer they look, the more accurate the test.
LoQ – a favourite acronym of us exposure geeks. It stands for Limit of Quantification, but what does that mean? It’s a threshold describing the sensitivity of the test: in effect, the analysts are saying ‘We don’t know exactly how much asbestos is there, but if it were above this number we would have found it all.’
All air tests have a LoQ which varies depending on the specifics of the test: how hard the pump was working (the sample rate), how long the test continued, and how many graticules were inspected. The more air you sample and the harder you examine it, the more sensitive the test is. If you find less asbestos than the LoQ (including none at all), you can’t be sure of this – so you say it was below the limit.
Back to the table. In a change from the existing analysts’ guide, you’ll see there are now four personal monitoring tests. Here’s what they’re for:
Four-hour Control Limit – this is a duty-of-care report: the employer is legally required to do these to demonstrate that individual workers are not exposed to asbestos above a certain limit, over a long period of time. That limit is 0.1 fibres per millilitre of air (f/ml) over four hours.
What you might not realise is that this is inside the RPE that you have provided. The other thing to remember is that these are tests associated with the individual being exposed – not the activity. So when analysing the data, make sure it is person-focused. I’ll go into more detail on these dreaded four-hour time-weighted average (TWA) tests later.
Ten-minute short-term exposure limit – this is the second legally mandated duty of care report. This test is intended to measure short-duration, high-intensity activity, and the limit is 0.6 fibres / ml inside the mask. Essentially this test is to detect brief ‘spikes’ in asbestos concentration, even when the average over four hours was acceptably low.
It’s very hard to achieve meaningful results in these tests. It’s obviously easy for the operative to be ‘painfully careful’ for 10 minutes, avoiding the kind of activity that might have otherwise produced a spike.
Assessment of suitability of RPE – this aims to gauge whether the mask was good enough for the task. This is related to the protection factor (PF) of the masks. To calculate it, you divide the exposure by the PF to identify the likely level inside the mask. Well-fitted, powered full-face masks give a protection factor of 40. Orinasal masks are rated at 20. Simple.
Specific short-duration activity (SSDA) – this is the ‘new’ kid on the block. I say ‘new’ as despite it not being on the list before, it is also the test standard that most licensed asbestos removal contractors (LARCs) try to achieve. It is essentially a test of how effective the method was.
The good news is that it is now on the list. The bad news is that the HSE has stated a sample rate of four litres per minute. Having spoken to the authors I can assure you that they mean up to four. Hopefully this typo will be amended before publication.
It’s my understanding that the HSE views the two most important tests from this list to be the four-hour control limit, and the SSDA. Indeed, now that SSDAs are on the list we will be able to remove one of the biggest problems to completing personal monitoring: analysts. More specifically, that many analysts do what the guidance tells them without exercising a deeper understanding.
Often, when a personal monitoring test is booked, an analyst concludes that they can’t do the four-hour test because the operative isn’t in the enclosure that long. Instead, they do the 10-minute test, the LoQ for which is so high as to be next to useless. This has been driving the HSE quietly mad for years, but now, when you are booking a personal, you can request a ‘SSDA Personal’.
I hope this will solve the problem, but it doesn’t get away from the lack of understanding surrounding the four-hour test, how to apply it, and how to calculate the results. As promised, we need to dive into them.
The dreaded four-hour time-weighted average tests
As I mentioned, the four-hour TWA tests are the main duty-of-care tests that we are legally mandated to do. They follow a World Health Organisation method which assures a level of accuracy that we would all agree is important when we are talking about people’s long-term health.
We do them because it’s the law, but more importantly because high-accuracy testing is the right thing to do. This is unfortunately easier to say than do. The rules are not widely understood, and the maths underpinning the test is fiendish. So here’s my attempt to simplify the whole topic.
Firstly it is better to think of the four-hour TWA as a calculation, not a test. The rules are that the test underpinning the calculation must look like this:
That brings us to the second and most important point: you don’t need to do a single four hour air test to calculate a valid four-hour TWA. Obviously running the air test for four hours will make the maths easier – but it is not essential. As long as the initial test is for two litres per minute and is run for at least two hours, we’re in business. What makes up the rest of the four hours can therefore come down to estimates and assumptions.
Squaring the circle
To explain this further, let’s look at a chart that the HSE presented at last year’s FAAM conference:
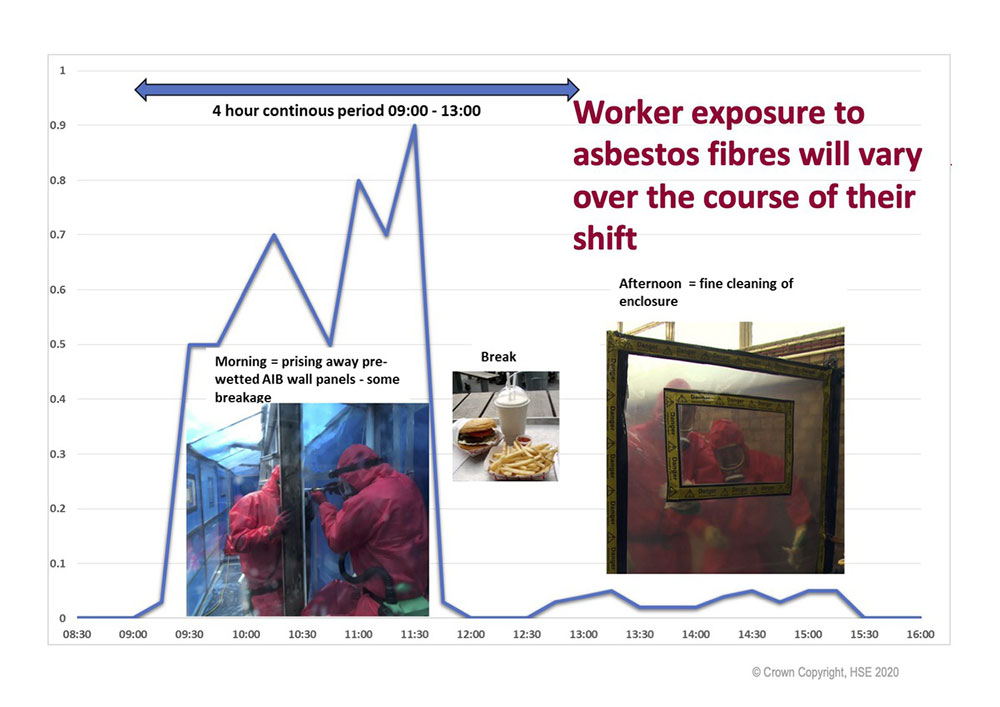
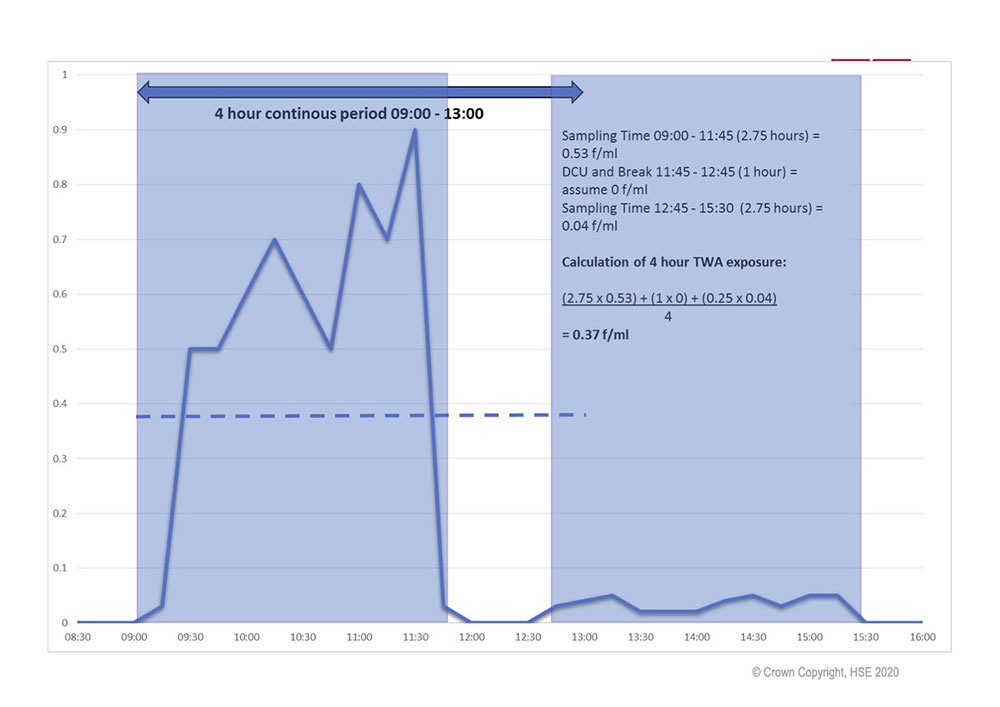
The aim is to capture the highest exposure (the initial removal phase) within the four-hour test. But it’s often the case that this doesn’t last for four hours. A second HSE chart helps show how you square the circle:
Charts by kind permission of Sam Lord HSE.
The activity is split into three distinct phases:
On this last bullet – there is a tantalising opportunity. Due to the very low impact of such a short low exposure event, it may be possible to build up a library of test results to populate the last bit of the calculation. But as only tests that comply with the basic WHO rules count, you may have to wait a while to build up the evidence. I have long advocated that the standard test should be one-hour long with a flow rate of two litres per minute. This gives us a decent level of accuracy for short-duration activity tests. If we increase this to two hours as standard, every test we do can be used for any of the HSE’s test categories.
The calculation (and why you don’t have to do it)
I’m going to take you through the steps to do the calculation by hand. But at this stage I should give you a spoiler alert: later in this post I’ll explain that Assure360 can do it all for you!
In the HSE’s example above, the equation is formed from three different work/rest sessions, and what proportion of the four-hour period they take up. As I mentioned – I have rounded the numbers to make it easier:
This gives us:

The trick is to do each of these as separate little sums and add them together (remember zero multiplied or divided by anything is zero):
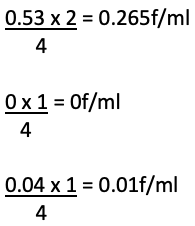
This gives you an answer of 0.275f/ml for the four-hour TWA.
If you’ve got the computing skills, you can create a spreadsheet that will do all of that for you. Alternatively it can be done by hand every time. But while the former is bad enough, the latter is quite soul destroying.
Making it simple
Those of you who’ve read my articles before will know that trying to simplify personal monitoring for LARCs could be considered ‘my thing’. I wanted to add my support to the HSE’s renewed push on personal monitoring, so we’ve added a new TWA tool to the Assure360 solution. Just as with everything else we do, a small tweak to the front end allows the system to do the heavy lifting for you – saving hours.
Our Paperless app has now been enhanced so that, along with the test result, it will collect three more data points:
The Assure360 database will do everything else for you. It will check the rules to make sure the test qualifies, and it will automatically do the calculation. Every test will be given its four-hour TWA value, and every duty-of-care report will provide the information.
If you are able to specify that all personal monitoring tests are at least two hours long with a flow rate of two litres per minute, it will also automatically start to build up a library of results that could be used to estimate the balance of any exposure
By automating calculation of the four-hour TWA, I hope that we can help ensure that more four-hour tests are carried out, and fewer mistakes and misunderstandings made. Improving the depth and quality of personal monitoring will, I hope, help the HSE reduce exposure in our industry, and improve working conditions for us all.
Want to see first-hand how Assure360 Paperless simplifies the four-hour TWA? Why not get in touch to book a free demonstration?
The Analysts’ Guide was finally published in May 2021. Click here to download it from the HSE website.
Tweet Share on Facebook Share on Linkedin